
Here. Hold my Asian American Teacup
Part Five: Last post in my ongoing series about Asian Americans
(Part One begins here)
If there is anything “good” to come from Asian stereotypes, it’s that most Asian ethnicities practice (for the most part) patience and respect for others; they believe that family is important above all else (with maybe the exception of religion). Perhaps it has to do with China being one of the oldest civilizations in the world that this trait had passed on to each ethnicity, but there is no doubt that certain mindfulness techniques (meditation, yoga, tai chi, for example) have derived from these Asian practices. [i]
I find it ironic that Western culture has latched onto these techniques; with gusto over the past several years, may I add. Yoga studios everywhere. Tai Chi being offered at Community Centers. Mindfulness techniques through meditation (think Headspace, Insight Timer, Calm). Which I think is a good thing; we all have to find a way to cope with anxiety and stress.
Then you have movies & TV shows, where they make (or in some cases remake) movies without using the appropriate actors. Hollywood has been notorious for “white-washing” many characters that should be Asian.
The release of the movie version [ii] of “Crazy Rich Asians” in 2018 was the first movie since the All-Asian, English-speaking cast of 1993’s “The Joy Luck Club.” That’s a 25-year difference and should give anyone an idea of how much Asian disparity there is in Hollywood-produced films.
Marvel Studios faced criticism from Asian Americans when Tilda Swinton was cast as The Ancient One in “Dr. Strange.” Whereas in the Marvel Comics, The Ancient One is a Tibetan man living in a hidden village on the Himalayan mountains. Swinton’s portrayal; however, is believed to be an androgynous Celtic woman.
There’s the casting of Scarlett Johansson as the main character in the Japanese manga & movie, 2017’s “Ghost in The Shell.” David Carradine’s “Kung Fu” series that ran from 1972 to 1975. [iii] Or the 2015 movies “Aloha” which stars Emma Stone as Allison Ng in “Aloha.” And “The Great Wall” where Matt Damon is depicted as the “white savior.”
As for the OG “Karate Kid” movies, I must say that – as 80’s as it was – at least they got the ethnicity correct (Japanese) with Mr. Miyagi. But the same can’t be said for the remake. That movie was based in China, when Karate is Japanese. Although, these days English-speaking individuals tend to use Karate for any or all Asian martial arts.
The most reviled “yellow face” in movies is Mickey Rooney in “Breakfast at Tiffany’s.” Mr. Rooney was cast as Mr. Yunioshi, the bumbling “oriental” (there’s that word again!) of Japanese descent. Time period or not, there are still recent movies utilize something called “Orientalism“ (a whole litany of that word!).
By definition, Orientalism is the way the Western world perceives Asia; where the concept of one’s ideas of an Asian person both exaggerates and distorts the Asian culture to define the differences between their white culture. It’s seen as a means to reinforce the positive image that non-Asians have of themselves while – at the same time – portraying Asians as odd, baffling, and sometimes barbaric. It’s a notion that the Western world is the epitome of humanity and that their morality, progress, power is superior to no one else. They see the Eastern world as a direct opposite of their “New World” ideals.
That said, patience and respect is something that all Asian & Asian Americans are taught at an early age. We are taught to respect our elders and recognize “hard work” as a way of success. We are taught in a subtle way to practice empathy; though it usually is disguised as being called “selfish.” [iv]
Most first-generation Asian Americans are taught that we should assimilate to American culture. Many of which were never taught their native language (<waves hand>) for fear that it would confuse (in my case) Tagalog with American English. In the case of many half-generation Asian Americans, they may be old enough to understand and/or speak in their native tongue. However, many are taught to only speak English at home; to practice the language to sound less like a foreigner with an accent. [v]
In particular, first-generation Asian Americans are taught to not “make waves.” That we shouldn’t cause a scene or make an issue about actions or behaviors that would ostracize their family and/or their culture. Meanwhile, in American culture, making waves is something more like making progress and/or change. [vi]
For those reasons (and many more), Asians & Asian Americans are seen and referred to as the “Silent Minority.” By definition, silent minority is a small number of people within a demographic group, or even the entire group (in this case, Asian & Asian Americans) who do – or rather will not – express their opinions publicly.
By doing this, the Silent Minority individual(s) choose to disassociate themselves from other groups (other ethnicities including Caucasians) on any hotly debated issue such as political or religious discussions, for example. They choose to be an inactive bystander by remaining neutral and not siding with either end of any particular topic.
In other words, it’s seen as a reason not to “rock the boat” while simultaneously showing that they are willing to assimilate to the American culture in order to be accepted.
There is another term that coexists with Silent Minority; one that likely encompasses what their silence is hoping to achieve. “Model Minority“ is defined as a minority group whose members (let’s say in this case, Asian Americans) wish to achieve a higher degree of socioeconomic or professional success in order to prove they are willing and able to be part of mainstream society.
For example, they strive for higher education believing that this will result in a prominent profession in which they can be a respected leader. They try to assimilate to remain neutral on hot topics (Silent Minority). They aim for a higher place in the socioeconomic ladder of the Western world so that they’d no longer feel judged by who (their ethnicity) and what (values, cultural practices, for instance) they are.
It’s these reasons that White America identify Asian Americans as a “model” for other ethnicities. This stem from their perception that Asian Americans we are less of a “threat” to their society by remaining neutral. They assume that Asian Americans do not want to share their thought on topics like racism, politics, and religion. They expect that Asian Americans will NOT speak up or participate in certain events. For example, the #MeToo organization. The #HumanRights, #LGBTQ, and #LoveIsLove campaigns. The #BlackLivesMatter and #SocialJustice movement. [vii]
Though white America believes that it’s a compliment to be labeled as a “model minority,” most Asian Americans (even if they remain silent) do not.
Asian Americans, especially GenX (and beyond), see this as an excuse to justify the exclusion of minorities as well as marginalize any individual success within a minority group (Prime example: “Asians are ALL smart”). Furthermore, this concept of being a Model Minority ultimately results in other marginalized groups pitting themselves against each other; where one groups believes they are able to assimilate and/or or be accepted into the American mainstream than the other group(s).
To me, this illustrates the reason why many of our immigrant parents (and other families & friends), remain neutral / side with popular white America. And why, despite being minorities themselves, they perceive all other ethnicities (Asian-, African- Americans and Latinos, for example) as being inferior to them. Much like how white America deems everyone inferior to them.
Personally, I find it pitiful that white America feels they need to set other minority groups against each other. This shameful behavior belongs in the middle school playground; not in the adult world. [viii]
What’s that term? “Divide and conquer”?
Look back at history, specifically the periods of civil unrest, the increase in hate crimes, and the onset of excessive verbal abuse from white America happened at a time of fear. Specifically, the fear that non-white Americans are a threat to their way of life. Fear of unemployment; of having their jobs “replaced” with a person who does not look like them. Fear of being “taken over” by other minorities.
Just like they feared the Filipino farm workers in Stockton were taking their jobs (and their women) from them. Or how during WWII, Japanese Americans were considered a threat to national security. Or how Vincent Chin died because two laid-off white autoworkers felt that any Asian (regardless of ethnicity) was responsible for the economic downfall of the Big Three.
Just like the 91-yo Filipino American in Oakland, CA seen by circuit TV was thrown to the ground. And the Asian American New Yorkers who have been spit on and verbally abused on the subways and streets of NYC.
Or the 83-yo Chinese woman in San Francisco who was punched without provocation and fought back. [ix] Additionally, she insisted that the remaining donations (around $900K) on GoFundMe given back to the AAPI community to combat racism and hate crimes. How’s that for a gesture of good will?
Just like the 8 people (six of them Asian) that were fatally shot at two different Asian spas by a 21-yo male with a supposed porn addiction. And the subsequent statement from the Chief of Police who marginalized those deaths by saying that he was just having a “really bad day.”
Again, all these incidents stem from fear and are perpetuated by stereotypes. All of these activities continue to occur because of anger. This anger ultimately surfaces with hate and hate crimes.
This is the moment where I state my favorite quote. This quote, IMHO, is a perfect analogy [x] on how hate crimes begin and its resulting outcomes. And yes, it’s from the very wise, 990-year-old Grand-master Jedi, Yoda.
“Fear is the path to the Dark Side.
Fear leads to Anger. Anger leads to Hate.
Hate leads to suffering.”
This is why I choose to speak up about Asian-American Hate Crimes, especially its part in US history. I feel it’s important for every resident in US to realize that Asians (and other non-white Americans), have always been seen as inferior to white person. That even though over the last 6 years, there has been a 150% increase in Asian Hate Crimes, these sentiments, behaviors, and actions have existed here in the US as far back as 1587 when Filipinos took those first steps in present-day Morro Bay, CA — 33 years before the Pilgrims landed at Plymouth Rock. And most definitely occurred before 1776, when the Declaration of Independence, which states that “All men are created equal“ was signed.[xi]
I’m speaking up about Model Minority because it pits Asian Americans and other ethnic groups against each other. Because it marginalizes any success that we achieve. Because it no longer pays to “assimilate” or strive to be better than other ethnicities. Because White America will always see us as inferior to them.
Because even though we’re acceptable, we are not accepted.
I’m speaking up because I no longer want to be a Silent Minority. I want it known that white America’s ethnically related behaviors and actions cause suffering. That this suffering not only affects Asian Americans but the United States as a whole [xii] And like many 1st & 2nd generations of Asian Americans, we want our voices to be heard.
We want to talk and debate about the disparities and inequities in OUR country. We want to discuss how Asian Americans and all other minority groups want social justice, equity, and equality for everyone in the US, regardless of race, religion, economic status, sex, gender, marriage, identity, etc
I’m speaking up because I want to help #StopAsianHate
I hope you take all that I’ve written to heart. My wish is that you pass on this knowledge to the next person and the next person and the next person. Because, if we don’t TALK ABOUT IT, nothing will ever change. And history, once again, would be doomed to repeated.
<Drops mic and walks off Soapbox>
[i] Now before you say that yoga derived from India and meditation had its beginnings as an Islam practice, both are rooted in Asian culture, as India and Saudi Arabia (where Islam began) are part of the Asian continent.
[ii] IMHO the movie, though very entertaining, does not compare to reading the book. (Although the mahjong scene at the end was a great addition.)
[iii] Though syndication of “Kung Fu” had even us 80’s kids watching it
[iv] Who am I kidding? Not only are we taught that we’re selfish as kids, but that thought of “being selfish” extends to our adult lives.
[v] Never mind that the parents still speak their language to you, you still had to respond in English
[vi] Does the whole “feeling I’m split in two make more sense now?
[vii] Seriously, I could go on and on and on …
[viii] NEWSFLASH: They will continue to do this unless something CHANGES. Which means talking about it.
[ix] Don’t mess with any Asian-American woman. We may look docile and agreeable, but – if pushed hard enough (both literally AND figuratively) – we strike back!
[x] Then again, this quote can be used in any situation
[xi] It also said that we have the right to vote. Thomas Jefferson when writing & signing the Declaration of Independence wrote, “Governments are instituted among Men, deriving their just Powers from the Consent of the Governed.” Just saying …
[xii] Think of why America was called “The Melting Pot” and why our Statue of Liberty reads:
“Give me your tired, your poor,
“The New Colossus” by Emma Lazarus
your huddled masses yearning to breathe free,
the wretched refuse of your teeming shore.
Send these, the homeless, tempest-tost to me,
I lift my lamp beside the golden door!”
 All Asians are NOT smart. They are NOT all doctors, nurses, engineers, or accountants. All Asians do NOT pass every test with A’s.
All Asians are NOT smart. They are NOT all doctors, nurses, engineers, or accountants. All Asians do NOT pass every test with A’s. 
 If you can recall, in the late 70’s and early 80’s, the auto industry was in a slow, unequivocal free fall. The energy crisis had hit the industry particularly hard. Since Detroit is known as the “Motor City,” the birthplace of mass-produced cars, many autoworkers were facing wage-cuts and/or job eliminations.
If you can recall, in the late 70’s and early 80’s, the auto industry was in a slow, unequivocal free fall. The energy crisis had hit the industry particularly hard. Since Detroit is known as the “Motor City,” the birthplace of mass-produced cars, many autoworkers were facing wage-cuts and/or job eliminations.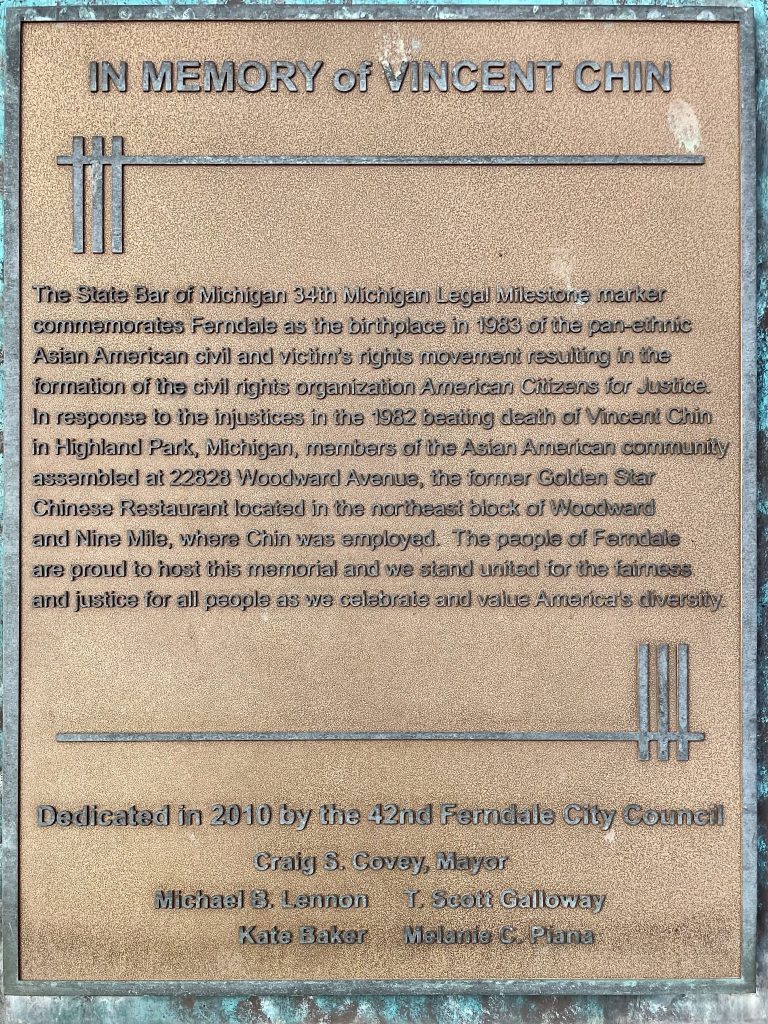 Ebens & Nitz spent 20 minutes looking for Chin, even paying another man $20 to help them find him. Chin was eventually found at a McDonald’s location close by. Nitz held Chin down as Ebens repeatedly bludgeoned Chin with the bat until his head split open. Sadly, Chin died 4 days later, never having gained consciousness. He was due to marry his fiancé later at the end of June.
Ebens & Nitz spent 20 minutes looking for Chin, even paying another man $20 to help them find him. Chin was eventually found at a McDonald’s location close by. Nitz held Chin down as Ebens repeatedly bludgeoned Chin with the bat until his head split open. Sadly, Chin died 4 days later, never having gained consciousness. He was due to marry his fiancé later at the end of June.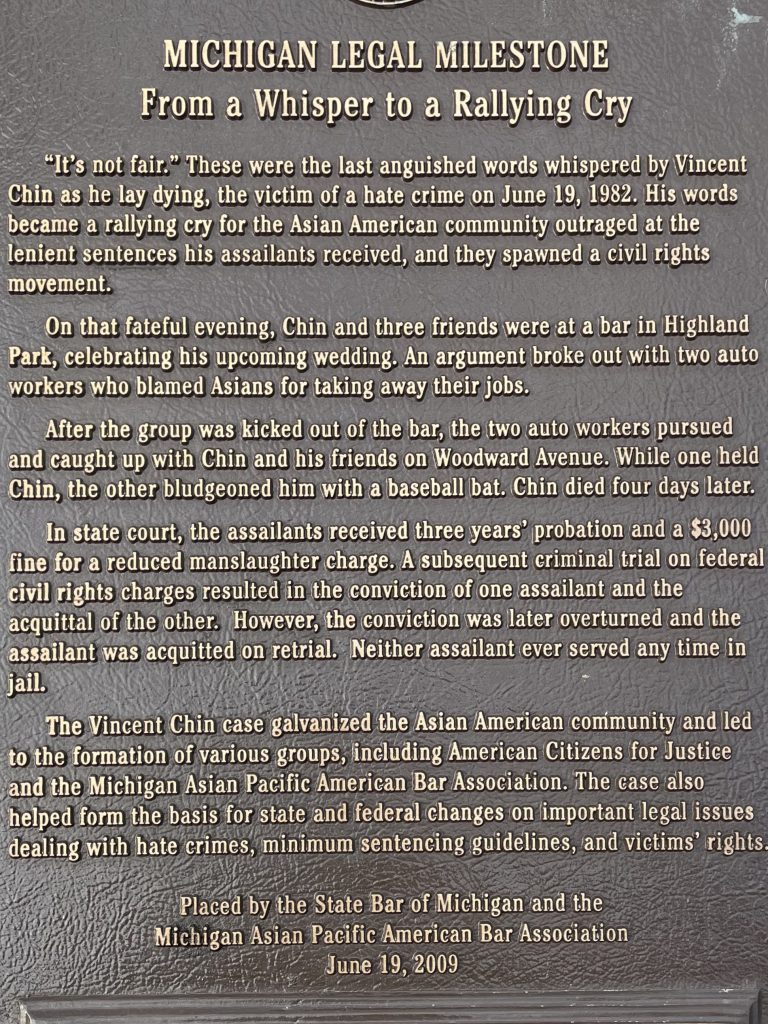 Vincent Chin is far from being the
Vincent Chin is far from being the  Growing up in the 80’s, I was labeled every kind of Asian celebrity out there; from Margaret Cho to Ming Na Wen (in her Joy Luck Club days, not the Agents of SHEILD days). Later it would become Sandra Oh or Lucy Lui. Any other person out there may have thought it was a compliment to be compared to beautiful actresses. For me, those “compliments” felt as if I was just viewed as an object in non-Asian persons’ eyes.
Growing up in the 80’s, I was labeled every kind of Asian celebrity out there; from Margaret Cho to Ming Na Wen (in her Joy Luck Club days, not the Agents of SHEILD days). Later it would become Sandra Oh or Lucy Lui. Any other person out there may have thought it was a compliment to be compared to beautiful actresses. For me, those “compliments” felt as if I was just viewed as an object in non-Asian persons’ eyes.
